If your ultrasound journey has begun you may have frequent headaches!
Ultrasound can be very subjective! Protocol is important to prevent that ominous feeling that your image series does not make sense. Subjective findings can cause one to lose focus on the study at hand and there are few things worse for a new sono than not knowing where to begin, continue or end a study.
I performed a foot exam today on a middle-aged woman with pain radiating from forefoot into her toes. Pain was elucidated somewhere in the region of the 2-4 MT heads. I have struggled to visualise interdigital neuroma. I want to share my strategy.
My protocol has been to :-
1. Dorsal foot- image each MTP jt in long to assess for ganglion/s, jt effusion , bony abnormality and simple assessment of the extensor tendons. Foot is flat down on table.
2. Dorsal assessment in longitudinal section - assess each webspace with leg straight and foot slightly dorsiflexed . Push the thumb of the non-transducer hand in to the plantar webspace while assessing dorsally to attempt visualisation of a morton's neuroma ( hypoechoic, heterogenous, oval, non-compressible perineural fibrosis), intermetatarsal bursitis (compressible).
3. Plantar foot- transducer in short axis in a coronal scan plane between metatarsal heads . Assess each webspace with dorsal compression. Label each MT head. Once again we are looking for that non-compressible hypoechoic and oval lesion between the MT heads, intermet bursitis and adventitial bursitis. Hopefully we can pop it out with compression to visualise well. The patient can assist in conveying any elucidated pain or discomfort.
4. Plantar foot - assess each webspace in long section . Again with the dorsal compression.

5. Plantar foot- assess each plantar plate and flexor tendon
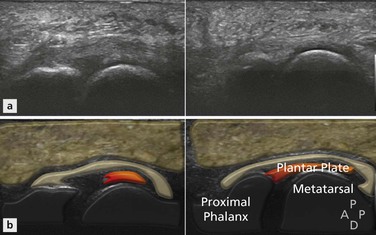
Image courtesy http://radiologykey.com/disorders-of-the-ankle-and-foot-forefoot/
Practice makes perfect. Protocol preparation means that you can focus on obtaining images and hopefully picking up pathology rather than trying to figure out how to best image and document your images.
On a different note just to finish:
A great sono told me when dealing with general masses take 3 trans, 3 long , 3 colour! Ensure your field of view is deep enough to assess the mass in relation to neighboring structures
FOR EXAMPLE - today I performed a groin US on a man 5 weeks post melanoma removal from ankle. Several lymph nodes were removed from the ankle, popliteal fossa and groin. Immediately deep to the groin scar was a hypoechoic nodule I felt was a round and unhappy lymph node with loss of focal fatty hilum. There were adjacent prominent nodes with focal fatty hila. Patient had tenderness and noticed 5 days prior.
The CFA and CFV are immediately deep to the lesion. Note the increased depth offers perspective. Differential now includes a slow leak false aneurysm. There were some linear striations within the lesion which may indicate clotting. There was no internal colour flow or spectral doppler flow.

